
Enhanced Recovery After Surgery (ERAS) and Immunonutrition: An Evidence-Based Approach. Perioperative nutrition: Recommendations from the ESPEN expert group - Clinical Nutrition. Weimann A.

Braga M. Carli F. Higashiguchi T. Hubner M. Klek S. et al.ESPEN guideline: clinical nutrition in surgery.Clin Nutr. 2017; 36: 623-650Chernoff R. How Sweet Is This? A Review and Evaluation of Preoperative Carbohydrate Loading in the Enhanced Recovery After Surgery Model - Ackerman - 2020 - Nutrition in Clinical Practice. Preoperative carbohydrate loading is a contemporary element of the enhanced recovery after surgery (ERAS) paradigm.

In addition to intraoperative surgical and anesthetic modifications and postoperative care practices, preoperative optimization is essential to good postsurgical outcomes. What was long held as dogma, a period of prolonged fasting prior to the administration of anesthesia, was later re‐examined and challenged. Along with the proposed physiologic effects of decreasing the surgical stress response and insulin resistance, preoperative carbohydrate loading was also demonstrated to improve patient satisfaction and well‐being, without an increase in perioperative complications.
Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations: Acta Orthopaedica: Vol 0, No 0. Over the last 15 years, the systematic implementation of an evidence-based perioperative care protocol (“fast-track” or “enhanced recovery pathway”), such as that developed by the Enhanced Recovery After Surgery (ERAS) Society, has shown that hospital length of stay and complications can be reduced for a number of surgical procedures (Ljungqvist et al. 2017 Ljungqvist O, Scott M, Fearon K C.
Enhanced Recovery After Surgery: a review. JAMA Surg 2017; 152(3): 292–8. [Crossref], [PubMed], [Web of Science ®] , [Google Scholar]). For total hip (THR) and total knee replacement surgery (TKR), high-volume models have reduced length of stay from 4–10 days to 1–3 days, and outpatient surgery is possible for around 15% of patients in unselected cohorts within a socialized health systems (den Hartog et al. 2013 den Hartog Y M, Mathijssen N M, Vehmeijer S B. Reduced length of hospital stay after the introduction of a rapid recovery protocol for primary THA procedures. Evidence level—Low Alcohol Anemia. Nutrition in Surgery and Critical Care - DCRI. Nutrition in Surgery Podcast - DCRI. Perioperative dietary therapy in inflammatory bowel disease. American Society for Enhanced Recovery and Perioperative Qua... : Anesthesia & Analgesia. Perioperative malnutrition has proven to be challenging to define, diagnose, and treat.

Ordering a Normal Diet at the End of Surgery—Justified or Overhasty? Pre‐operative nutrition and the elective surgical patient: why, how and what? - Gillis - 2019 - Anaesthesia. Introduction In the peri‐operative period, the primary nutrition goals are to evaluate the patient for pre‐existing malnutrition, treat malnutrition to optimise surgical readiness, minimise starvation, prevent postoperative malnutrition, and support anabolism for recovery 1.
Although additional nutritional considerations will be required for surgical subspecialities and to provide personalised patient care, these basic nutrition principles hold true for all cases. Our paper uses Simon Sinek's Golden Circle approach 2 to apply these basic surgical nutrition principles to the pre‐operative period, largely focusing on elective abdominal surgery. Surgical stress response An understanding of the surgical stress response is essential to understanding the role nutrition plays in promoting optimal surgical recovery. Nutritionally‐relevant clinical consequences of the surgical stress response include hyperglycaemia and whole‐body protein catabolism 1, 2. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018.
Preadmission items See Fig. 1. 1.
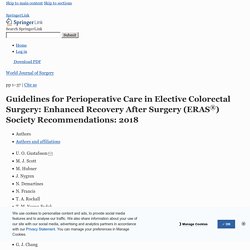
Preadmission information, education and counselling Comprehensive preoperative counselling has several important goals. An international consensus statement on the management of postoperative anaemia after major surgical procedures - Muñoz - - Anaesthesia. Consensus Statement on Nutrition Screening and Therapy Within a Surgical Enhanced Recovery Pathway. Role of nutrition support in adult cardiac surgery: a consensus statement from an International Multidisciplinary Expert Group on Nutrition in Cardiac Surgery. Cardiac surgery with myocardial ischemia/reperfusion and use of CPB is known to be associated with deleterious consequences, resulting from the inflammatory response during cardiac surgery.

The duration of CPB time correlates with the extent of the inflammatory response. Furthermore, surgical trauma, ischemia/reperfusion, and contact activation with the CPB circuit result in the release of mainly pro-inflammatory markers, reactive oxygen species, and reactive nitrogen species that contribute to the development of organ dysfunction [35]. In this setting, the use of pharmaco-nutrients, which may exert specific effects on metabolism, the inflammatory response, markers of oxidative stress, and immune cell activity, are of considerable interest.
The amino acids glutamine and arginine, lipids such as omega-3 fatty acids, micronutrients such as selenium and zinc, or vitamins A, C, D, and E, are examples of such key nutrients. Reducing Postsurgical Wound Complications: A Critical Review. The annual number of surgical procedures performed globally is growing, which emphasizes the need for proper management of postsurgical wounds.
According to the Centers for Disease Control and Prevention’s (CDC’s) national report, there were more than 157,500 surgical site infections (SSIs) associated with inpatient surgeries in 2011.1 This accounted for 31% of healthcare-associated infections among hospitalized patients. In addition, SSIs were associated with a 3% mortality rate and $10 billion in annual costs.1 Although progress has been made in the improvement of postsurgical patient outcomes, further reduction in morbidity and mortality can be accomplished with proper preoperative and postoperative precautions. This is especially true for patients at high risk of wounds and SSIs, such as those with diabetes or irradiated tissues.
In the current reimbursement system, avoiding these postsurgical complications and their progression to chronic wounds is paramount. Smoking Obesity. Guidelines for perioperative care after radical cystectomy for bladder cancer: Enhanced Recovery After Surgery (ERAS®) society recommendations. 8.Epidural analgesia (EDA) 9.Minimally invasive approach Minimally invasive pelvic surgery has been shown to decrease the inflammatory response when compared to the open approach.

Laparoscopic rectal surgery seems to reduce the risk of postoperative ileus, complications and length of stay. However, long term oncological results are awaited before any higher LE statement can be drawn. Three prospective case series studies evaluated some form of minimally invasive approach to radical cystectomy. 10.Resection site drainage 11.Antimicrobial prophylaxis and skin preparation Regarding the optimal skin preparation, the ERAS recommendations in elective colorectal are of absolute value in cystectomy patients. 12.Standard anesthetic protocol Attention should be paid to maintain normoglycemia (possibly blood sugar less than 10 mmol/l), and adequate lung ventilation with low tidal volumes to limit peak airway pressure thus reducing the risk of barotrauma. 13.Perioperative fluid management. ESPEN guideline: Clinical nutrition in surgery.
Recommendation 6: It is recommended to assess the nutritional status before and after major surgery.

Grade of recommendation GPP – strong consensus (100% agreement) Recommendation 7: Perioperative nutritional therapy is indicated in patients with malnutrition and those at nutritional risk. Perioperative nutritional therapy should also be initiated, if it is anticipated that the patient will be unable to eat for more than five days perioperatively. Enteral and Parenteral Nutrition in the Perioperative Period: State of the Art.