
Inguinal Hernia Repair : Monograph. By Rosalyn Carson-DeWitt, MD Anatomy and Physiology The abdominal wall consists of layers of skin, fat, muscle, fascia, and membranes.
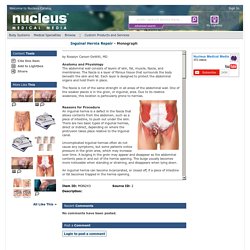
The fascia is a layer of fibrous tissue that surrounds the body beneath the skin and fat. Each layer is designed to protect the abdominal organs and hold them in place. The fascia is not of the same strength in all areas of the abdominal wall. One of the weaker places is in the groin, or inguinal, area. Reasons for Procedure An inguinal hernia is a defect in the fascia that allows contents from the abdomen, such as a piece of intestine, to push out under the skin. Uncomplicated inguinal hernias often do not cause any symptoms, but some patients notice pressure in the groin area, which may increase over time.
An inguinal hernia can become incarcerated, or closed off, if a piece of intestine or fat becomes trapped in the hernia opening. If a piece of intestine is incarcerated, the flow of materials inside the intestine can become obstructed. Academy of Medicine of Malaysia - General Guidelines. Inguinal hernia repair - NHS Choices. Introduction A hernia occurs when an internal part of the body pushes through a weakness in the muscle or surrounding tissue wall.
Your muscles are usually strong and tight enough to keep your intestines and organs in place, but a hernia can develop if there are any weak spots. Recovering from Open Hernia Repair: Patient Guide. TeachMeAnatomy - Making Anatomy Simple. Executive Summary - Surgical Options for Inguinal Hernia: Comparative Effectiveness Review - NCBI Bookshelf. Pyogenic and amebic liver abscess - Surgical Treatment - NCBI Bookshelf. Surgical Options for Inguinal Hernia: Comparative Effectiveness Review - NCBI Bookshelf. Enterocutaneous Fistulas: Enterostomal Therapy and Wound Care of the Enterocutaneous Fistula Patient. Necrotizing fasciitis secondary to enterocutaneous fistula: Three case reports. Www.casereports.com/article/S2210-2612(14)00347-2/pdf. Jscr.oxfordjournals.org/content/jscr/2014/11/rju121.full.pdf.
Controversy in inguinal hernia: seroma: occurrence, prevention, and management - WeBSurg, the e-surgical reference of Laparoscopic surgery. Size and position of the mesh - WeBSurg, the e-surgical reference of Laparoscopic surgery. Radiology Articles. General Surgery News - Current Issue. Atlas of Surgical Anatomy » Medical Books Free. Lecture Notes: General Surgery – 12th Edition » Medical Books Free. Www.e-mfp.org/old/2009v4n2_3/pdf/Breast_lesions.pdf# Surgery for early breast cancer - Early and Locally Advanced Breast Cancer - NCBI Bookshelf. Ductal Carcinoma In Situ of the Breast: A Surgical Perspective. British Journal of Cancer - The effect of DCIS grade on rate, type and time to recurrence after 15 years of follow-up of screen-detected DCIS. DCIS Test Identifies Patients With Low Recurrence Risk. Early and locally advanced breast cancer. The following guidance is based on the best available evidence.
The full guideline gives details of the methods and the evidence used to develop the guidance. 1.1 Referral, diagnosis and preoperative assessment Patients with symptoms that could be caused by breast cancer are referred by their GP to designated breast clinics in local hospitals (see NICE clinical guideline 27, 'Referral guidelines for suspected cancer'). In addition, women aged between 50 and 70 are invited for screening mammography every 3 years through the NHS Breast Screening Programme (NHSBSP) in England or the Breast Test Wales Screening Programme (BTWSP) in Wales. For most patients, whether they are referred following breast screening or after presentation to a GP, diagnosis in the breast clinic is made by triple assessment (clinical assessment, mammography and/or ultrasound imaging, and core biopsy and/or fine needle aspiration cytology).
Review of Internal Hernias: Radiographic and Clinical Findings : American Journal of Roentgenology: Vol. 186, No. 3 (AJR) TABLE 1: Clinical and Imaging Findings for Internal Hernias Left Paraduodenal Hernia Left paraduodenal hernias have an overall incidence of approximately 40% of all internal hernias.

They occur when bowel prolapses through Landzert's fossa, an aperture present in approximately 2% of the population (Fig. 1). These hernias therefore can be classified as a congenital type, normal aperture subtype. Landzert's fossa is located behind the ascending or fourth part of the duodenum and is formed by the lifting up of a peritoneal fold by the inferior mesenteric vein and ascending left colic artery as they run along the lateral side of the fossa. Right Paraduodenal Hernia Foramen of Winslow hernias often present a similar radiographic appearance to that of left paraduodenal hernias. Clinically, these hernias present as described, with no distinctive or characteristic findings on history or physical examination.
Address correspondence to W. 1. 5.