
Leukaemia caused by chromosome catastrophe. Researchers have found that people born with a rare abnormality of their chromosomes have a 2,700-fold increased risk of a rare childhood leukemia.

In this abnormality, two specific chromosomes are fused together but become prone to catastrophic shattering. Acute lymphoblastic leukemia, or ALL, is the most common childhood cancer. Scientists previously found that a small subset of ALL patients have repeated sections of chromosome 21 in the genomes of their leukemia cells. This form of ALL -- iAMP21 ALL -- requires more intensive treatment than many other types of ALL. The scientists used modern DNA analysis methods to reconstruct the sequence of genetic events that lead to iAMP21 ALL. The team noticed that some patients with iAMP21 ALL were born with an abnormality in which chromosome 15 and chromosome 21 are fused together. "We have been able to map the roads the cells follow in their transition from a normal genome to a leukemia genome. " Gene therapy cures leukaemia in eight days.
WITHIN just eight days of starting a novel gene therapy, David Aponte's "incurable" leukaemia had vanished.

For four other patients, the same happened within eight weeks, although one later died from a blood clot unrelated to the treatment, and another after relapsing. The cured trio, who were all previously diagnosed with usually fatal relapses of acute lymphoblastic leukaemia, have now been in remission for between 5 months and 2 years. Michel Sadelain of the Memorial Sloan-Kettering Cancer Center in New York, co-leader of the group that designed the trial, says that a second trial of 50 patients is being readied, and the team is looking into using the technique to treat other cancers.
The key to the new therapy is identifying a molecule unique to the surface of cancer cells, then genetically engineering a patient's immune cells to attack it. Engineered immune cells produce complete response in child with an aggressive leukemia. By reprogramming a 7-year-old girl's own immune cells to attack an aggressive form of childhood leukemia, a pediatric oncologist has achieved a complete response in his patient, who faced grim prospects when she relapsed after conventional treatment.
The innovative experimental therapy used bioengineered T cells, custom-designed to multiply rapidly in the patient, and then destroy leukemia cells. After the treatment, the child's doctors found that she had no evidence of cancer. Pediatric oncologist Stephan A. Grupp, M.D., Ph.D., of The Children's Hospital of Philadelphia, and colleagues from the University of Pennsylvania presented updated results of the clinical trial involving these engineered cells at the American Society of Hematology (ASH) annual meeting December 10 in Atlanta.
Grupp's research builds on his ongoing collaboration with Penn scientists who originally developed the modified T cells as a treatment for B-cell leukemias. New Culprit Discovered in T-Cell Acute Lymphoblastic Leukemia. January 11, 2012 - 4:30pm A new study published in the journal Nature Medicine by NYU Cancer Institute researchers, shows how the cancer causing gene Notch, in combination with a mutated Polycomb Repressive Complex 2 (PRC2) protein complex, work together to cause T- cell acute lymphoblastic leukemia (T-ALL).
T-ALL is an aggressive blood cancer, predominately diagnosed in children. It occurs when one lymphoblast, an immature white blood cell, turns malignant, multiplying uncontrollably and spreading rapidly throughout the body. If left untreated, the disease can be fatal in a few weeks. Cancer-causing Notch mutations in T-ALL are well established, yet the detailed molecular mechanism mediating this Notch-induced cancer cell transformation was unknown until now. The study shows a new dynamic interplay between Notch and PRC2 function. The study shows T-ALL as an epigenetic disease, regulated by a subtle equilibrium between oncogenes and tumor suppressors. Media Inquiries: Cancer Drugs Cure Now, May Cause Problems Later, UB Research Shows. BUFFALO, N.Y. -- Will a drug used to treat childhood acute lymphoblastic leukemia and other pediatric cancers cause heart problems later in life?

UB associate professor of pharmaceutical sciences, Javier G. Blanco, PhD, who sees his work as a bridge between research and clinical practice, has focused recent efforts on trying to answer this question. Blanco and colleagues' recent study in the Journal of Clinical Oncology looked for the underlying genetic answers to why some childhood cancer survivors who were treated with anthracylines -- powerful antibiotics like Adriamycin and Daunomycin -- developed cardiomyopathy, such as congestive heart failure, later in life.
"Anthracyclines are effective drugs used to treat a variety of pediatric cancers, they are also used to treat breast cancer and other malignancies in adults," Blanco says. "After cancer, survivors can develop cardiac toxicity anywhere from one year to more than 15 years after the initial chemotherapy with anthracyclines. Acute lymphoblastic leukemia. Cure is a realistic goal, as ≥94% of children have continuous disease-free survival for five years and appear cured, while 30–40% of adults have continuous disease-free survival for five years.
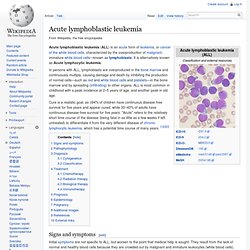
"Acute" refers to the relatively short time course of the disease (being fatal in as little as a few weeks if left untreated) to differentiate it from the very different disease of chronic lymphocytic leukemia, which has a potential time course of many years. [1][2][3] Signs and symptoms[edit] Initial symptoms are not specific to ALL, but worsen to the point that medical help is sought. They result from the lack of normal and healthy blood cells because they are crowded out by malignant and immature leukocytes (white blood cells). Therefore, people with ALL experience symptoms from malfunctioning of their erythrocytes (red blood cells), leukocytes, and platelets. The signs and symptoms of ALL are variable but follow from bone marrow replacement and/or organ infiltration.
Pathophysiology[edit] 1. I.