
Hyperpnea in Postural Tachycardia. Welcome Welcome to the Hyperpnea in Postural Tachycardia Study website.
Researchers at the Center for Hypotension at New York Medical College in Valhalla NY have received funding from the American Heart Association (AHA) to study the cause of increased breathing (hyperpnea) in postural tachycardia syndrome in teenagers and young adults. Our most recent data indicate that this is particularly associated with sympathetic activation in important subsets of POTS. The Principal Investigator is Dr. Julian Stewart What comprises the study population? What comprises the study population? We are seeking patients aged 18-29 years old with postural tachycardia syndrome (POTS) who may benefit from an investigation of abnormalities of regulation of respiration and sympathetic nervous system regulation. ^top. Sympathetic nervous system. Adrenergic receptor. The adrenergic receptors (or adrenoceptors) are a class of G protein-coupled receptors that are targets of the catecholamines, especially norepinephrine (noradrenaline) and epinephrine (adrenaline).
Many cells possess these receptors, and the binding of a catecholamine to the receptor will generally stimulate the sympathetic nervous system. The sympathetic nervous system is responsible for the fight-or-flight response, which includes widening the pupils of the eye, mobilizing energy, and diverting blood flow from non-essential organs to skeletal muscle. History[edit] Raymond Ahlquist, Professor of Pharmacology at Medical College of Georgia, published a paper concerning adrenergic nervous transmission in 1948[1] but its significance was largely ignored at that time. Categories[edit] There are two main groups of adrenergic receptors, α and β, with several subtypes. α receptors have the subtypes α1 (a Gq coupled receptor) and α2 (a Gi coupled receptor). Norepinephrine. Medically it is used in those with severe hypotension.
It does this by increasing vascular tone (tension of vascular smooth muscle) through α-adrenergic receptor activation. Areas of the body that produce or are affected by norepinephrine are described as noradrenergic. Epinephrine. Physiological effects[edit] The adrenal medulla is a minor contributor to total circulating catecholamines (L-DOPA is at a higher concentration in the plasma),[11] though it contributes over 90% of circulating epinephrine.
Little epinephrine is found in other tissues, mostly in scattered chromaffin cells. Following adrenalectomy, epinephrine disappears below the detection limit in the blood stream.[12] The adrenals contribute about 7% of circulating norepinephrine, most of which is a spill over from neurotransmission with little activity as a hormone.[13][14][15] Pharmacological doses of epinephrine stimulate α1, α2, β1, β2, and β3 adrenoceptors of the sympathetic nervous system. Sympathetic nerve receptors are classified as adrenergic, based on their responsiveness to adrenaline.[16] Vasoconstriction, Norepinephrine, and Fibromyalgia. Red Blood Cells and Chronic Fatigue Syndrome New Zealand researcher Dr.
L.O. Simpson has theorized that Chronic Fatigue Syndrome results from "insufficient oxygen availability due to impaired capillary blood flow. " Simpson attributes the impaired capillary blood flow to smaller-than-usual capillaries and to the presence of abnormal red blood cells. ("Red Blood Cells and Chronic Fatigue Syndrome") Vasoconstriction When the core body temperature is cooled below approximately 37 degrees Celsius (98.6 F), special mechanisms are set into play to conserve the heat that is already in the body, and still other mechanisms are set into play to increase the rate of heat production.
Pheochromocytoma. A pheochromocytoma (from Greek phaios "dark", chroma "color", kytos "cell", -oma "tumor") or phaeochromocytoma (PCC) is a neuroendocrine tumor of the medulla of the adrenal glands (originating in the chromaffin cells), or extra-adrenal chromaffin tissue that failed to involute after birth[1] and secretes high amounts of catecholamines, mostly norepinephrine, plus epinephrine to a lesser extent.[2] Extra-adrenal paragangliomas (often described as extra-adrenal pheochromocytomas) are closely related, though less common, tumors that originate in the ganglia of the sympathetic nervous system and are named based upon the primary anatomical site of origin.
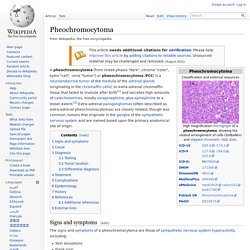
Signs and symptoms[edit] The signs and symptoms of a pheochromocytoma are those of sympathetic nervous system hyperactivity, including: A pheochromocytoma can also cause resistant arterial hypertension. A pheochromocytoma can be fatal if it causes malignant hypertension, or severely high blood pressure. Ghrelin. Ghrelin (pr.
GREL-in), the "hunger hormone", is a peptide produced by ghrelin cells in the gastrointestinal tract[1][2] which functions as a neuropeptide in the central nervous system.[3] Beyond regulating hunger, ghrelin also plays a significant role in regulating the distribution and rate of use of energy.[4] When the stomach is empty, ghrelin is secreted. When the stomach is stretched, secretion stops. It acts on hypothalamic brain cells both to increase hunger, and to increase gastric acid secretion and gastrointestinal motility to prepare the body for food intake.[5] History and name[edit] Ghrelin was discovered after the ghrelin receptor (called growth hormone secretagogue type 1A receptor or GHSR) was discovered in 1996[9] and was reported in 1999.[10] The hormone name is based on its role as a growth hormone-releasing peptide, with reference to the Proto-Indo-European root ghre, meaning to grow.[11] (Growth Hormone Release-Inducing = Ghrelin)